|
|
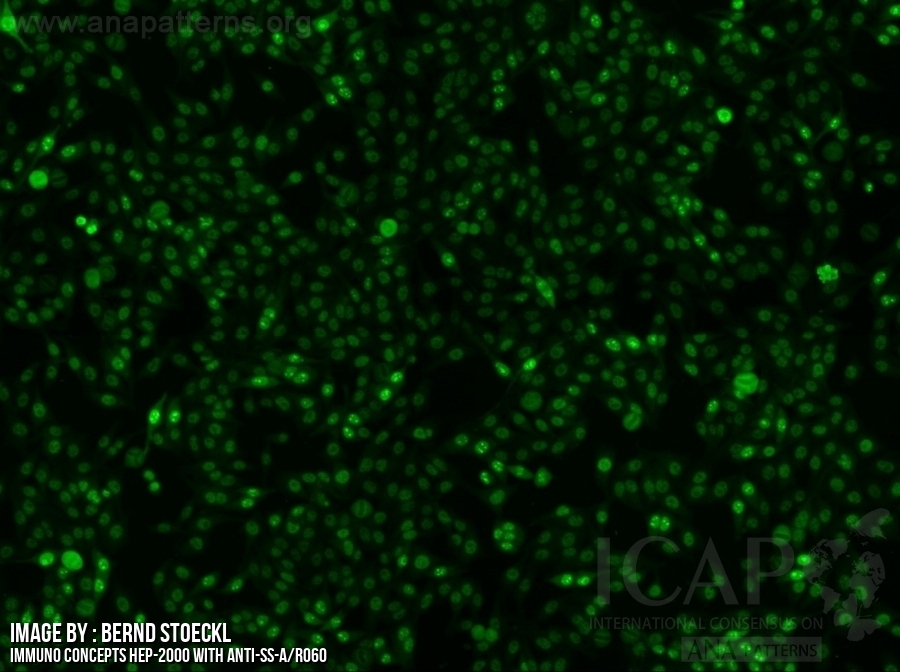
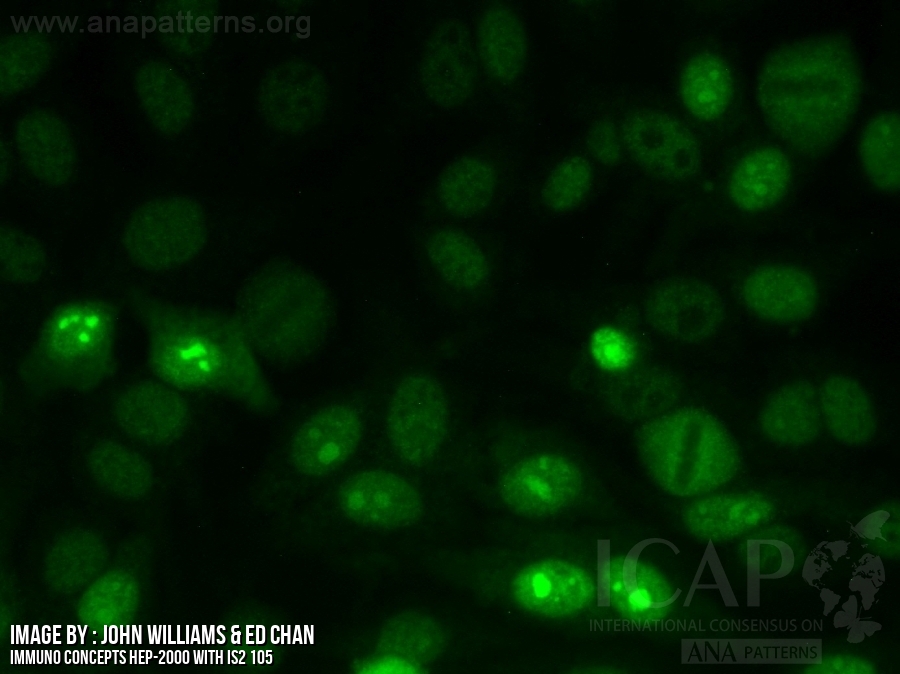
| Previous Nomenclature | fine granular |
| Description | Fine tiny speckles across all nucleoplasm. The nucleoli may be stained or not stained. Mitotic cells (metaphase, anaphase, and telophase) have the chromatin mass not stained. e.g. anti-SS-A/Ro, anti-SS-B/La |
| Antigen Association | SS-A/Ro, SS-B/La, Mi-2, TIF1γ, TIF1β, Ku |
|
Clinical Relevance
First level information About Clinical Relevance & List of Abbreviations |
|
▶ Present to a varying degree in distinct SARD, in particular SjS, SLE, subacute cutaneous lupus erythematosus, neonatal lupus erythematosus, congenital heart block, DM, SSc, and SSc-AIM overlap syndrome (15) ▶ If SjS, SLE, subacute cutaneous lupus erythematosus, neonatal lupus erythematosus, or congenital heart block is clinically suspected, it is recommended to perform follow-up tests for anti-SS-A/Ro (Ro60) and anti-SS-B/La antibodies; in most laboratories these antigens are included in the routine ENA profile (15) ▶ Autoantibodies to SS-A/Ro are part of the classification criteria for SjS (the criteria do not distinguish between Ro60 and Ro52/TRIM21) (25) ▶ If SSc, AIM, or to a lesser extend SLE, is clinically suspected, it is recommended to perform follow-up tests for detecting autoantibodies to Mi-2, TIF1γ, and Ku; these antigens are typically included in disease specific immunoassays (i.e., inflammatory myopathy profile*) (26) ▶ Autoantibodies to Mi-2 and TIF1γ are associated with DM; autoantibodies to TIF1γ in patients with DM, although rare in the overall AC-4 pattern, is strongly associated with malignancy in old patients (26, 27) ▶ Autoantibodies to Ku are associated with SSc-AIM and SLE-SSc-AIM overlap syndromes (26) Note: Anti-SS-A/Ro (Ro60) and AIM-specific autoantibodies may be undetected in HEp-2 IIFA-screening (28) *Availability of the inflammatory myopathy profile, the SSc profile and the (extended) liver profile may be limited to specialty clinical laboratories. |
| First level information references |
|
15. Conrad K, Schössler W, Hiepe F. Autoantibodies in systemic autoimmune diseases: a diagnostic reference. 2. 3th edn. Autoantigens autoantibodies autoimmunity, 2015. 25. Shiboski CH, Shiboski SC, Seror R, et al. American College of Rheumatology/European League against rheumatism classification criteria for primary Sjögren´s syndrome: a consensus and data-driven methodology involving three international patient cohorts. Ann Rheum Dis 2016;2017:9-16. 26. Betteridge Z, McHugh N. Myositis-specific autoantibodies: an important tool to support diagnosis of myositis. J Intern Med 2016;280:8-23. 27. Trallero-Araguás E, Rodrigo-Pendás JÁ, Selva-O´Callaghan A, et al. Usefulness of anti-p155 autoantibody for diagnosing cancer-associated dermatomyositis: a systematic review and meta-analysis. Arthritis Rheum 2012;64:523-32. 28. Bossuyt X, Frans J, Hendrickx A, et al. Detection of anti-SSA antibodies by indirect immunofluorescence. Clin Chem 2004;50:2361-9. |
| Second level information |
|
None |
| Second level information references |
|
None
|
| FAQ |
|
How to deal with just a “nuclear speckled” IFA report? In my practice I have followed patients with ANA findings, with a nuclear speckled pattern (without specifying whether fine/dense/coarse), in patients with very heterogeneous phenotypes, some with a clinical picture that suggests further investigation of systemic autoimmune disease (one patient with proximal muscle weakness and skin thickening) and others who represent only non-specific findings. In such situations, as a precaution, I request more specific autoantibodies. However, this pattern (nuclear speckled pattern) is not described by the "ICAP" and I am in doubt about which antigenic association it represents, even to guide which autoantibody may be present and which ones to look after. How to interpret this pattern? Does the lab describe it when it is not possible to "refine" such a conclusion? Could this be associated with deficiency in the methodology, sample, interpretation?
Tips to identify AC-4a pattern True IFA staining masked at low dilution? Question: In the IFA testing of a 9-year-old female lupus patient, initial dilution at 1/40 produced a bright fuzzy cytoplasmic staining with no well-defined pattern. Surprisingly nuclear fine speckled AC-4 was observed at 1/160. Is it common that the cytoplasmic staining completely masked the nuclear staining at low dilution? Anti-Ro52 antibodies with an AC pattern? Do anti-Ro52 antibodies show any staining pattern matching with known ICAP AC designation? I have a patient with exclusive anti-Ro52 +++ (strong) in immunoblot and I do not know which AC pattern it should correspond to. AC-4? AC-XX? Ro/SS-A and La/SS-B negative in HEp-2 IFA. Can I get positive Ro and La with negative ANA IFA? How to explain if yes? |